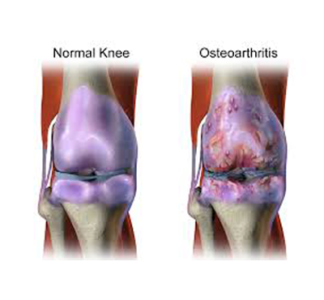
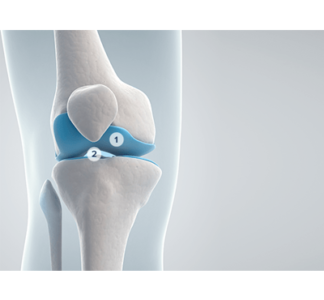
So you have osteoarthritis of the Knee. What can you do about it?
Osteoarthritis (OA) is the most common joint disorder in the world. OA affects the majority of people
over the age of 65 and is recognized as one of the leading causes of disability in the elderly.
There are 2 major risk factors that have been found for OA of the Knee:
- Age – prevalence of OA increases with age; 14% of adults aged 25 and older have OA, while 34% will have OA after the age of 65.
- Obesity – The risk of getting knee OA is approximately double the risk of those who are of normal weight or underweight.
Other factors include:
Systemic factors: increasing the vulnerability of the joint
- Gender (female > male)
- Bone density
- Nutritional factors
- Genetic predisposition
Local Mechanical factors:
- Malalignment
- Muscle weakness
- Alterations of the structural integrity of the joint (eg. Meniscal damage, ACL tear, etc.)
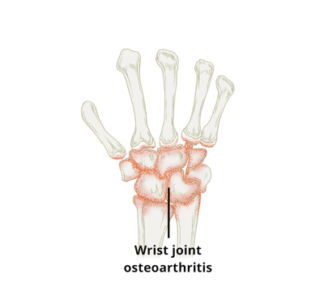
The most common sites of Osteoarthritis include:
- Hand – 70%
- Spine – 60%
- Knee – 30%
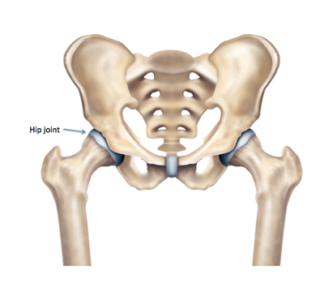
- Hip – 10%
OA rarely occurs in the ankle, shoulder and elbows (except after trauma).
How to recognize the characteristic symptoms of Osteoarthritis
- Pain in mechanical in nature – it occurs with activity and relieved with rest.
- usually subtle in onset.
- 3) Morning stiffness is absent or lasts < 30 minutes. One gets short periods of stiffness after inactivity.
- Crepitus
- Joint swelling
- Reduced range of motion
- Bony enlargement of the joint
- Joint deformity
- Instability/laxity of the joint
- No palpable warmth of joint
Not all of these symptoms may appear.
Management – What can we do?

The aims of management include
- Patient education about the disease and its management
- Pain control
- Improve function and decrease the disability
- Alter the disease process and its consequences
For the purpose of this article lets talk about some non-pharmacologic knee OA management strategies. At this point in time, there is evidence that these do help:
- Patient education
- Arthritis Self-ManagementProgram
- Personalized social support
- Weight loss
- Aerobic exercise
- Physiotherapy
- Muscle-strengtheningexercises
- Assistive devices forambulation
- Patellar taping
- Appropriate footwear
- Joint protection and energyconservation
- Assistive devices foractivities of daily living
- Tai Chi programs
- Traditional Chineseacupuncture
- Transcutaneous electrical Stimulation (TENS, IFC)
Weight Loss
It is very important to lose weight through a combination of diet and exercise.
Increased BMI has been associated with an increased prevalence of knee, hip, and hand OA.
Weight loss of 5 kg is associated with a 50% reduction in chance of developing OA and also slows progression.Felson DT, Zhang Y. Arthritis Rheum. 1998.
Gudbergsen H, Boesen M, Lohmander LS, et al. Weight loss is effective for symptomatic
relief in obese subjects with knee osteoarthritis independently of joint damage severity
assessed by high-field MRI and radiography. Osteoarthritis Cartilage. 2012;20(6):495–
502.
This study showed the following effects of a 16-week weight-loss regime on symptomatic
relief in an elderly and obese group of patients:
An improvement of 14% on the knee injury and osteoarthritis outcome score (KOOS)
A 64% response rate on the OARSI/outcome measures in rheumatology (OMERACT)
criteria independent of structural damage at baseline, muscle strength, and alignment.
Exercise
Exercise increases aerobic capacity, muscle strength, and endurance
(these also facilitate weight loss).
All persons capable of exercise should be encouraged to participate in a
low-impact aerobic exercise program (walking, biking, swimming, aquatic
exercise, Tai chi).
Quadriceps strengthening exercises have been shown to lead to
improvements in pain and function:
Messier SP, Loeser RF, Miller GD, et al. Exercise and dietary weight loss in overweight
and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion
Trial. Arthritis Rheum. 2004;50(5):1501-1510.
Ettinger WH Jr, Burns R, Messier SP, et al. A randomized trial comparing aerobic
exercise and resistance exercise with a health education program in older adults with
knee osteoarthritis. The Fitness Arthritis and Seniors Trial (FAST). JAMA.
1997;277(1):25-31.
Messier SP, Mihalko SL, Beavers DP, et al. Strength Training for Arthritis Trial (START):
design and rationale. BMC Musculoskelet Disord. 2013;14(1):208.
Adherence to exercise and physical activity is vital for long-term benefits.
Jordan JL, Holden MA, Mason EE, Foster NE. Interventions to improve adherence to
exercise for chronic pain in adults. Cochrane Database Syst Rev. 2010;1: CD005956
stimulation
Knee braces
Randomized trials of the effectiveness of braces for the treatment of medial knee OA demonstrate
that wearing an unloader knee brace gives a clinically significant and immediate improvement in the pain and function, approximately 50%, of patients with medial osteoarthritis of the knee, which is much
more than seen with typical NSAIDs prescription. Kirkley A, et al. J Bone Joint Surg Am. 1999.









 Ask A Question
Ask A Question
 Get Clinical Pricing
Get Clinical Pricing
 Health Hub
Health Hub
 Shipping Policy
Shipping Policy
 Returns/Exchanges
Returns/Exchanges
 About Us
About Us
 Contact Us
Contact Us
 Login | Register
Login | Register